In order to acquire the highest level of evidence to answer a clinical question, researchers need access to credible and established information resources. Researchers should make inquiries with their peers and colleagues regarding the types of evidence resources that are available. If researchers do not have access to clinical evidence at the point of care, then they have to make a decision as a professional to invest money into keeping up-to-date with current practice standards. Criteria were set forth that will help you in making this decision.*
If researchers are asking a background question as defined in the previous section of the EBM decision tree, then existing electronic and paper textbooks such as Harrison's, MDConsult, UpToDate, and Stat!Ref can be used.
If researchers are asking a foreground question as defined in the previous section of the EBM decision tree, then the foundation of their search terminology and subsequent search queries should be built around the research question as it is operationalized by the PICO mnemonic.
MeSH headings should be used in the literature search queries. To look up current MeSH headings, click on this link: http://www.nlm.nih.gov/mesh/
If researchers are asking a background question as defined in the previous section of the EBM decision tree, then existing electronic and paper textbooks such as Harrison's, MDConsult, UpToDate, and Stat!Ref can be used.
If researchers are asking a foreground question as defined in the previous section of the EBM decision tree, then the foundation of their search terminology and subsequent search queries should be built around the research question as it is operationalized by the PICO mnemonic.
MeSH headings should be used in the literature search queries. To look up current MeSH headings, click on this link: http://www.nlm.nih.gov/mesh/
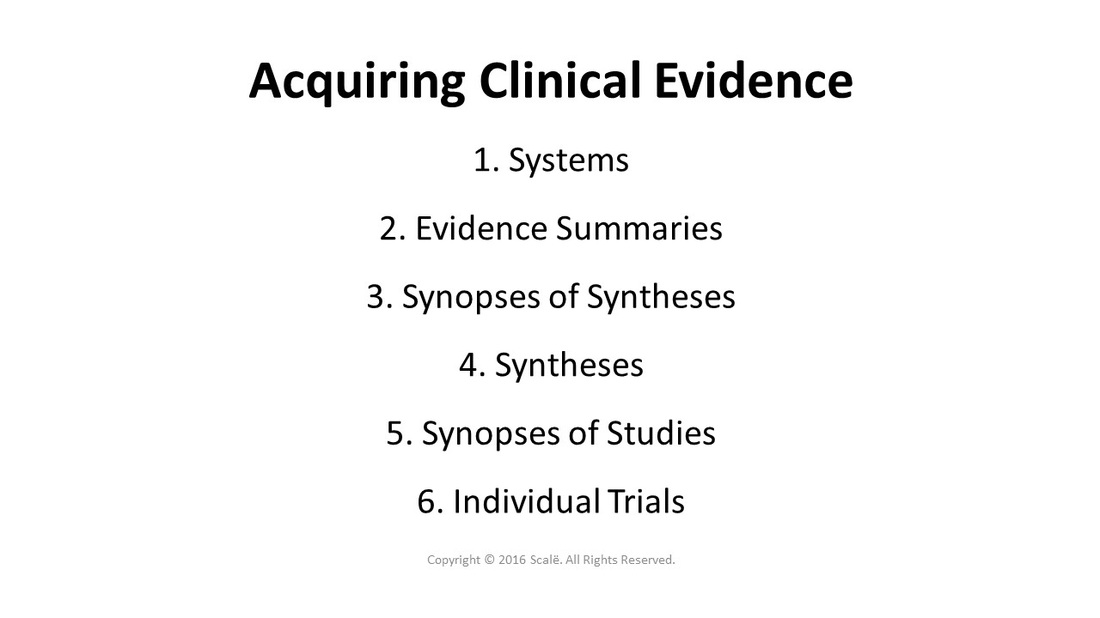
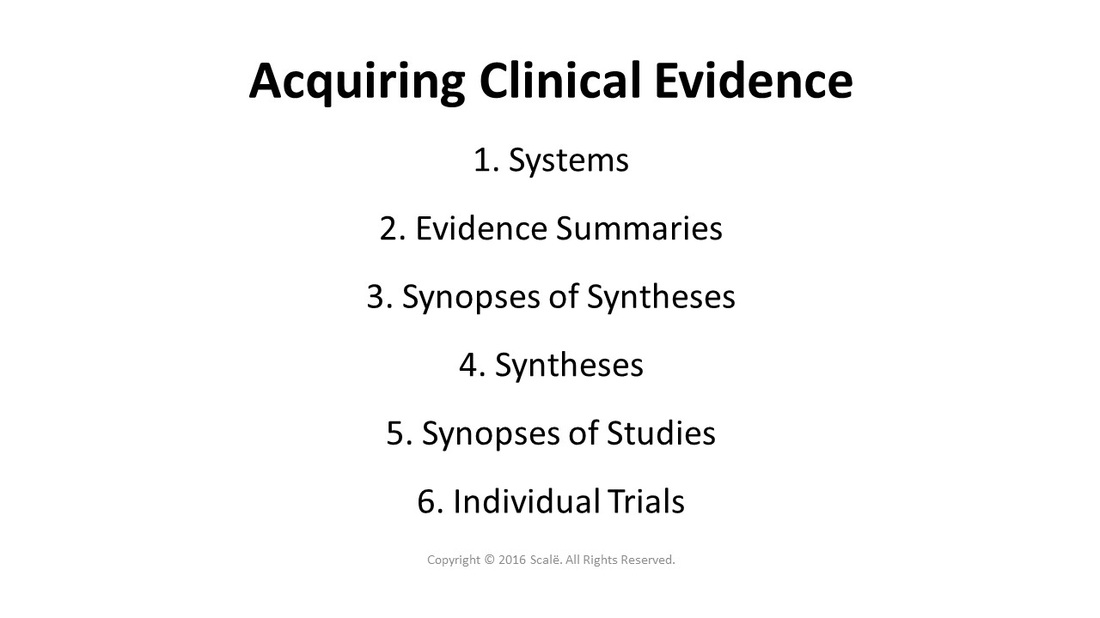
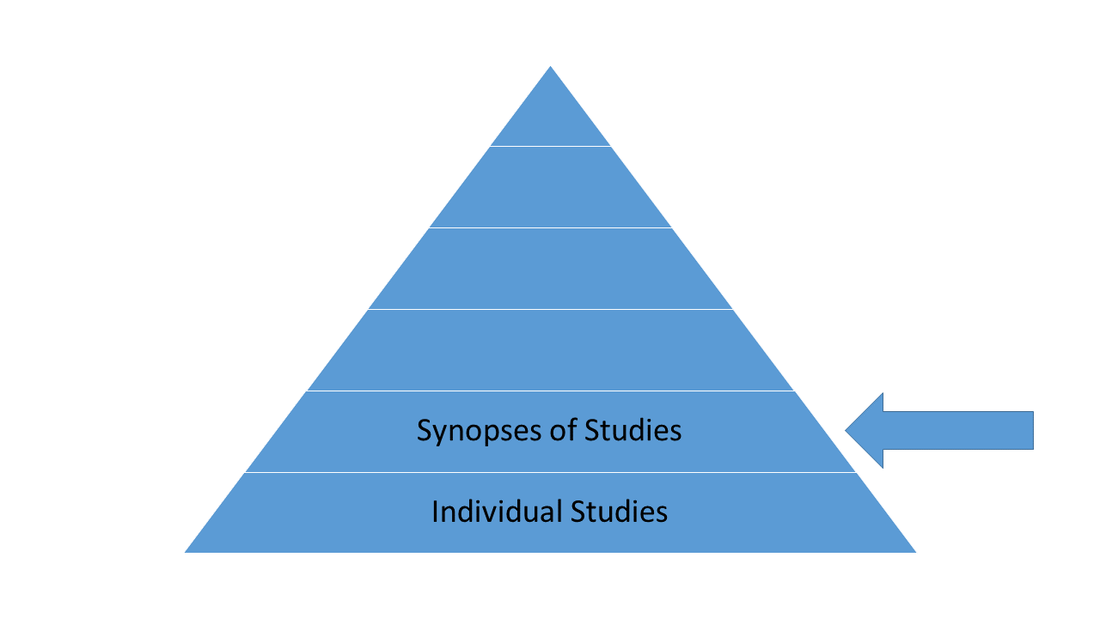
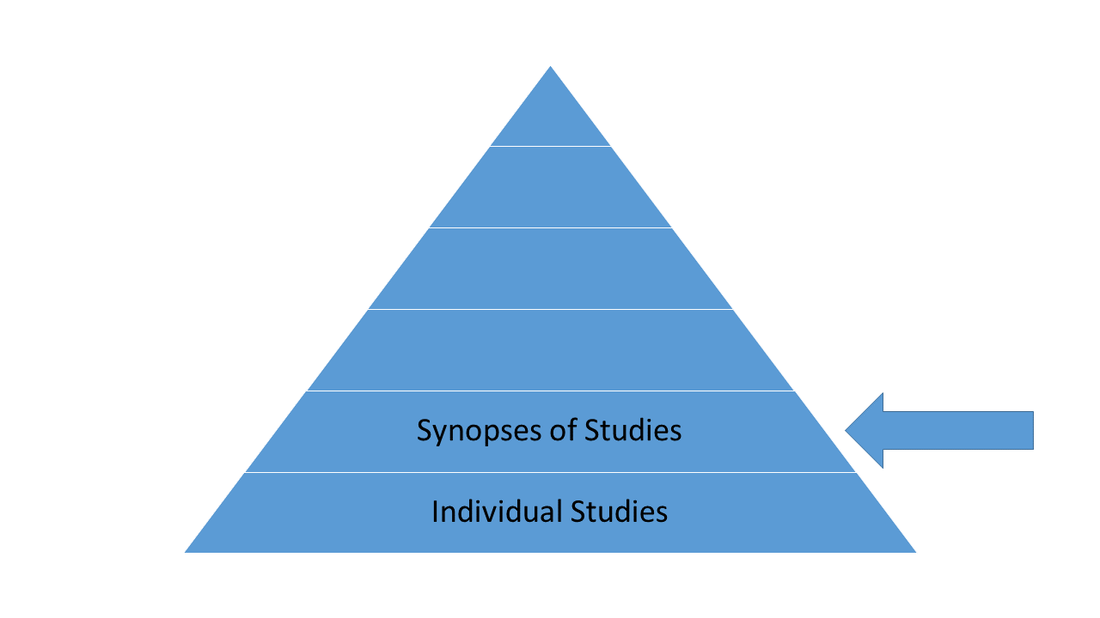
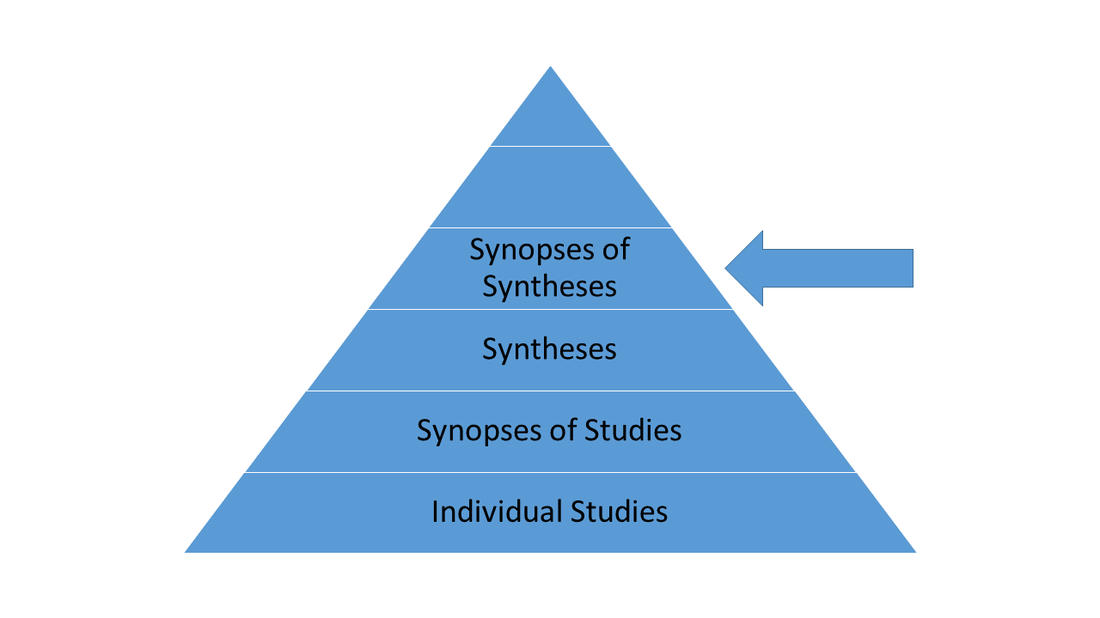
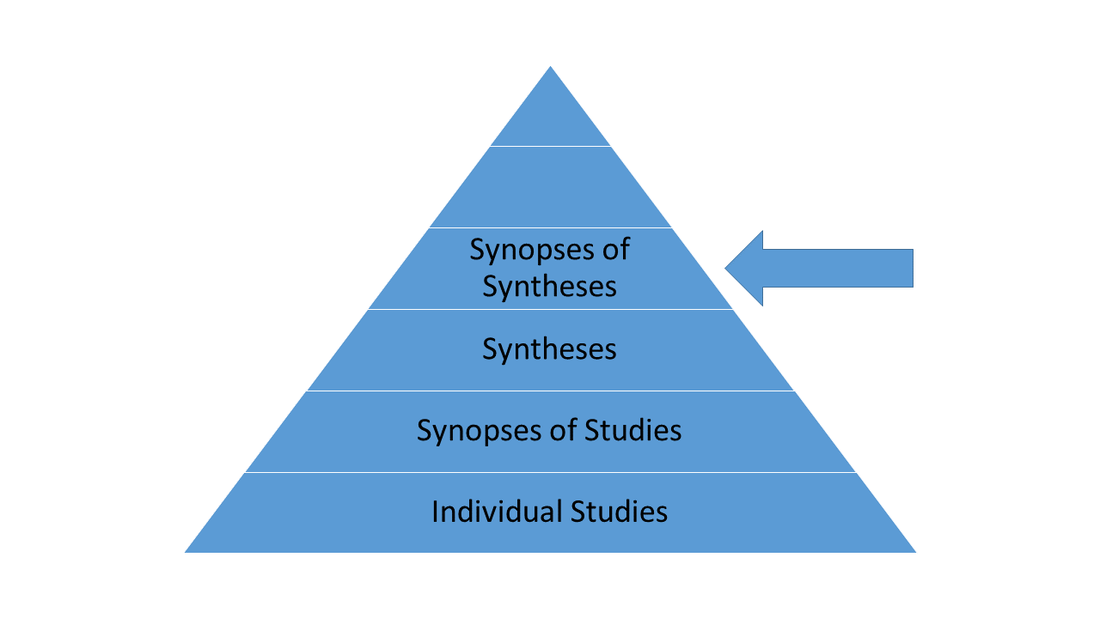
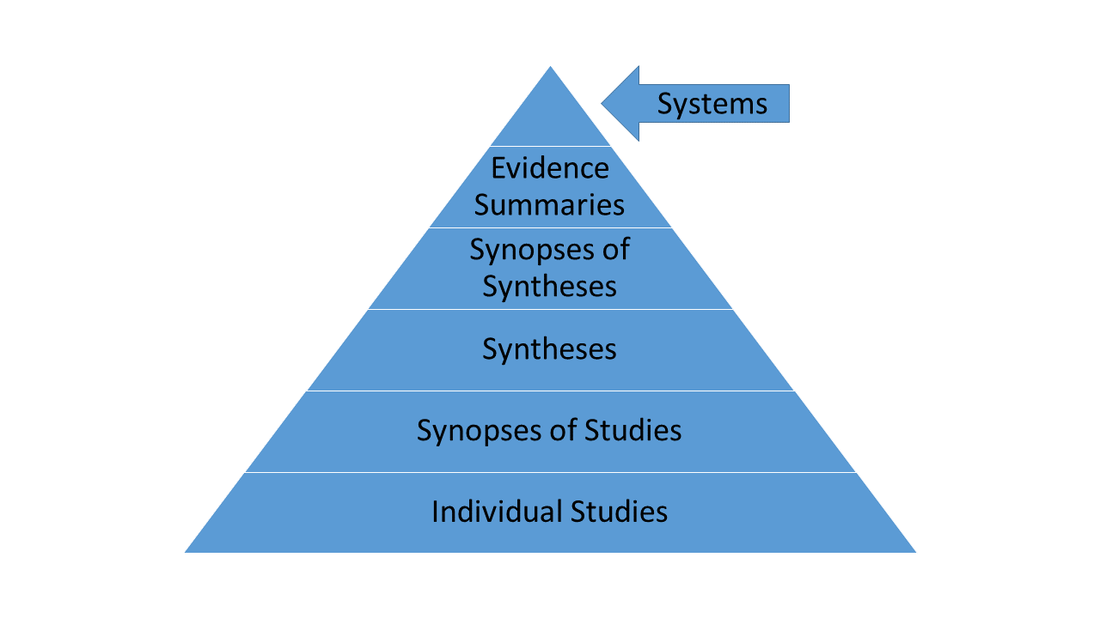
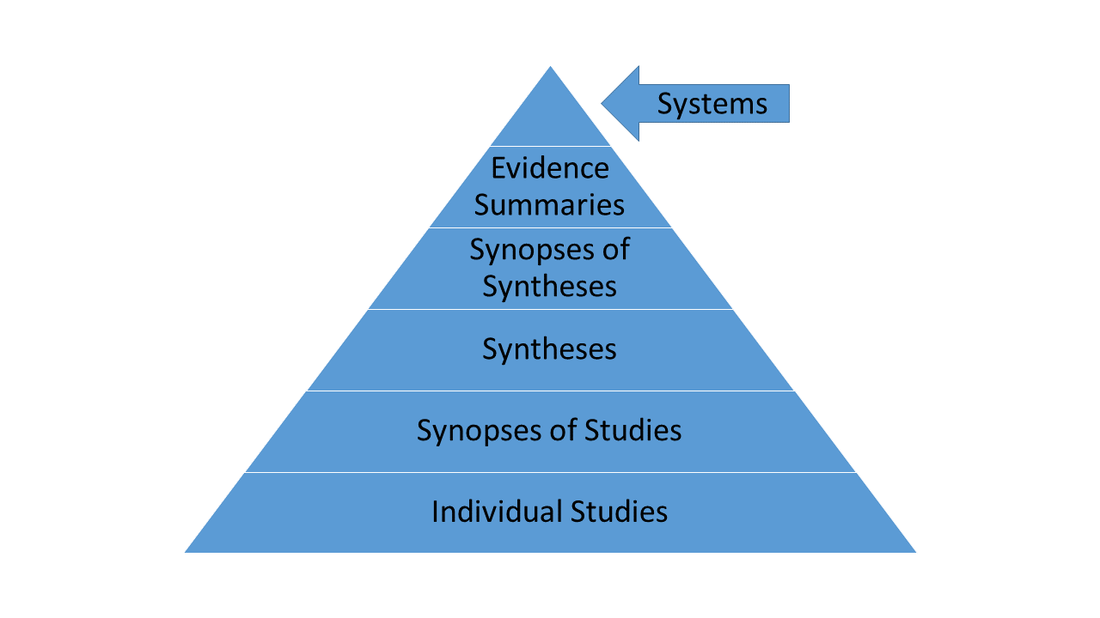
There are six levels of evidence in EBM practice.** Lower levels of evidence should only be accessed if higher tiered evidence does not exist or cannot be acquired.
The lowest level of evidence is the individual RCT. While these studies constitute the highest level of applied experimental science, when applying clinical evidence to actual patients in the clinical environment, a higher standard of "empirical" care is essential. This should be the last resort after conducting multiple literature searches and not finding any pertinent higher level evidence. Look for sensitivity analyses in the article that are applicable to the client. Observational studies should rarely be used.
The second echelon of evidence is synopses of studies. These synopses are highly validated summaries of pre-appraised RCTs that are published and delivered in a practical and concise format to clinicians.
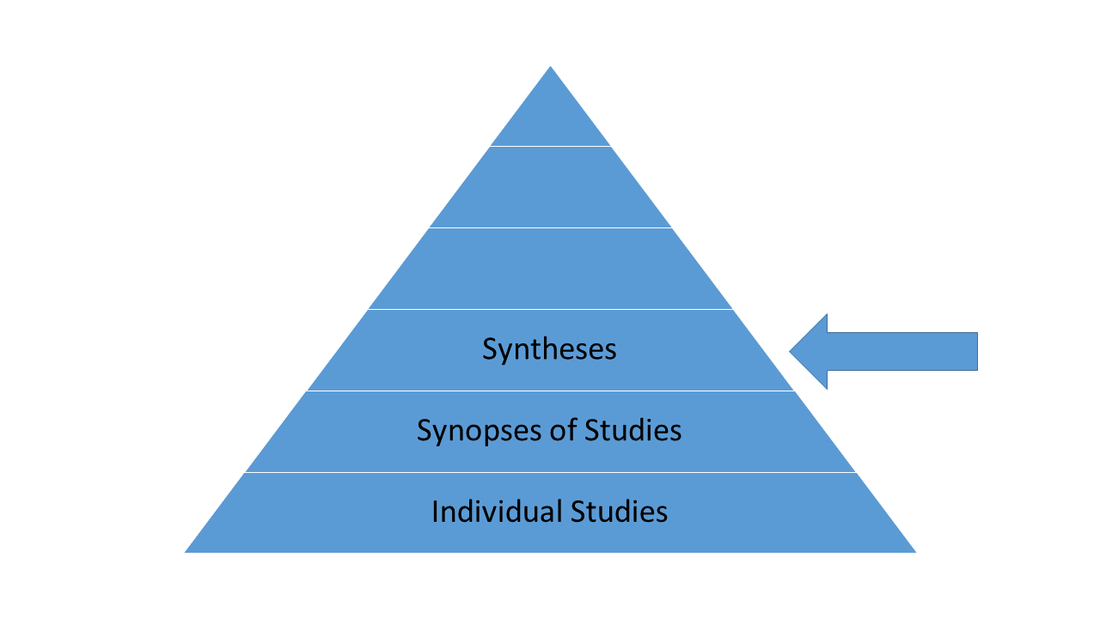
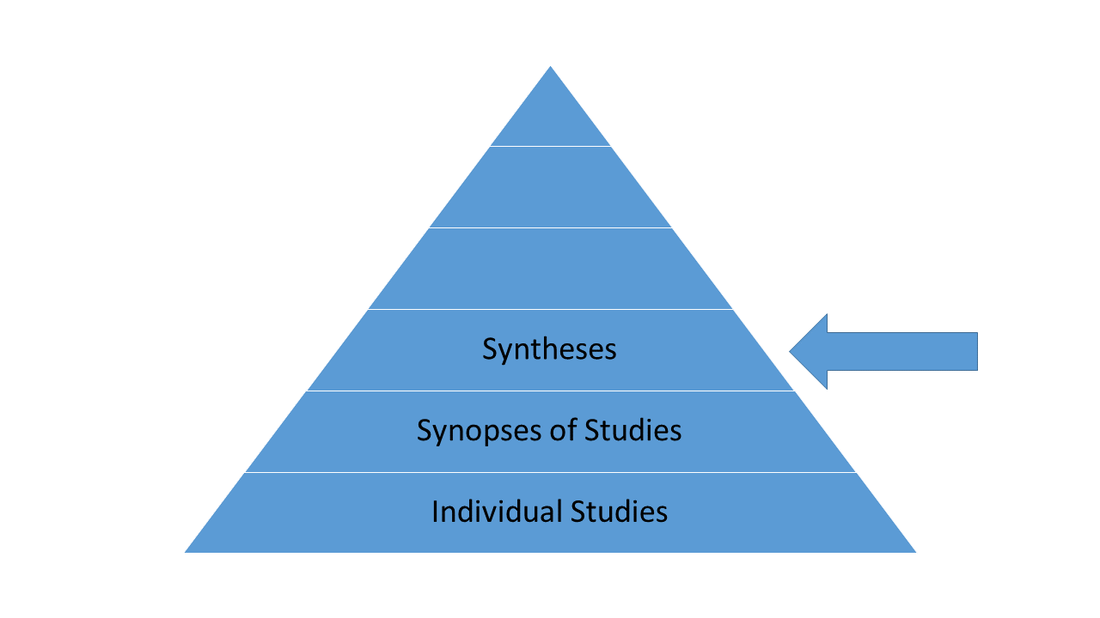
The third level of evidence of evidence consists of syntheses of treatment effects yielded from rigorous systematic reviews.
The fourth tier of evidence consists of synopses of syntheses, which are highly validated summaries of pre-appraised systematic reviews that are published and delivered in a practical and concise format to clinicians.
The fifth level of evidence is comprised of summaries of synopses related to individual disease states, treatments, differential dx, and therapy.
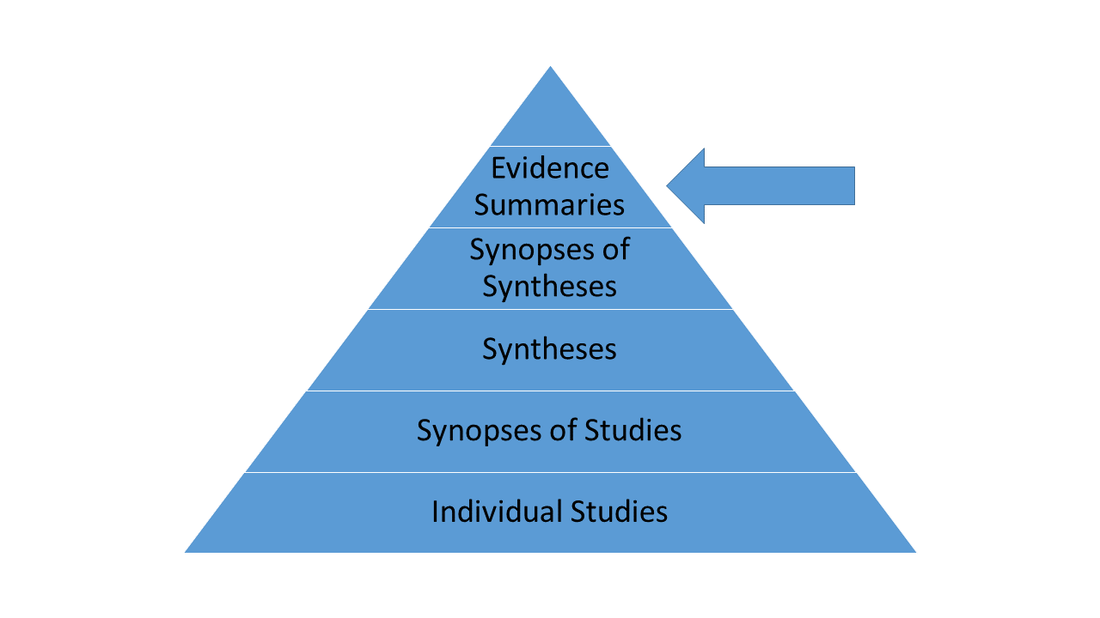
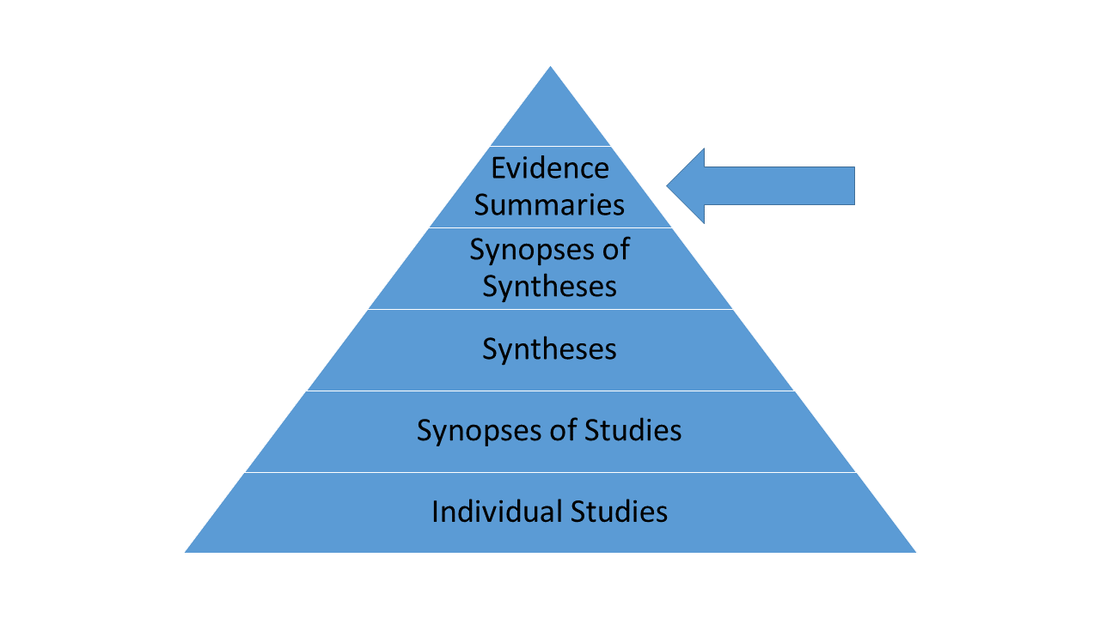
This level of evidence does not currently exist. It posits direct and seamless integration of relevant high-level clinical evidence into the patient's electronic medical record (EMR) as patient data is entered. Evidence will be automatically integrated into the patient chart as data is entered.
Click on the Appraising Clinical Evidence button to continue.
*Guyatt G, Rennie D, Meade MO, Cook DJ. Users' guides to the medical literature: A manual for evidence-based clinical practice. Chicago: AMA press; 2008
**Straus SE, Glasziou P, Richardson WS, Haynes RB. Evidence-based medicine: How to practice and teach it. Edinburgh: Churchill Livingstone; 2011
**Straus SE, Glasziou P, Richardson WS, Haynes RB. Evidence-based medicine: How to practice and teach it. Edinburgh: Churchill Livingstone; 2011